Informing U.S. engagement with the world

The Latest in U.S.-China AI Competition
By Michael Froman
India’s Cockroach Party Protests Have a Powerful Precedent—and It Isn’t the Arab Spring
By Sadanand Dhume

Will Iran Turn Into a Forever War?
By Ray Takeyh

CFR Surveyed 350 Experts About AI’s Future. Here Are the Takeaways.
By Jessica Brandt and Adam Segal
AI’s Economic Winners
By Rebecca Patterson


Iran War’s Ripple Effect
 Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert TakeNavigating the AI Moment
 Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert Take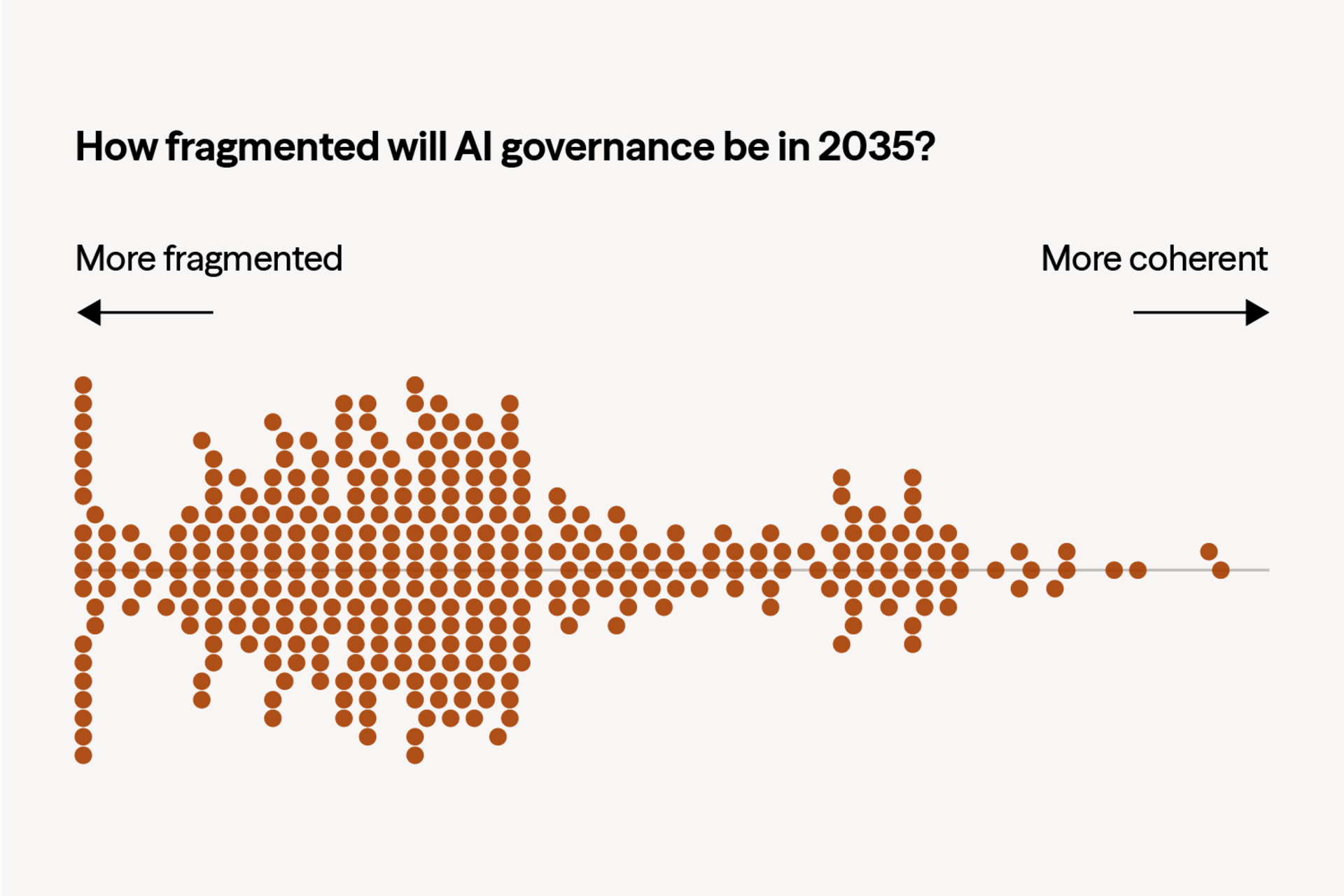
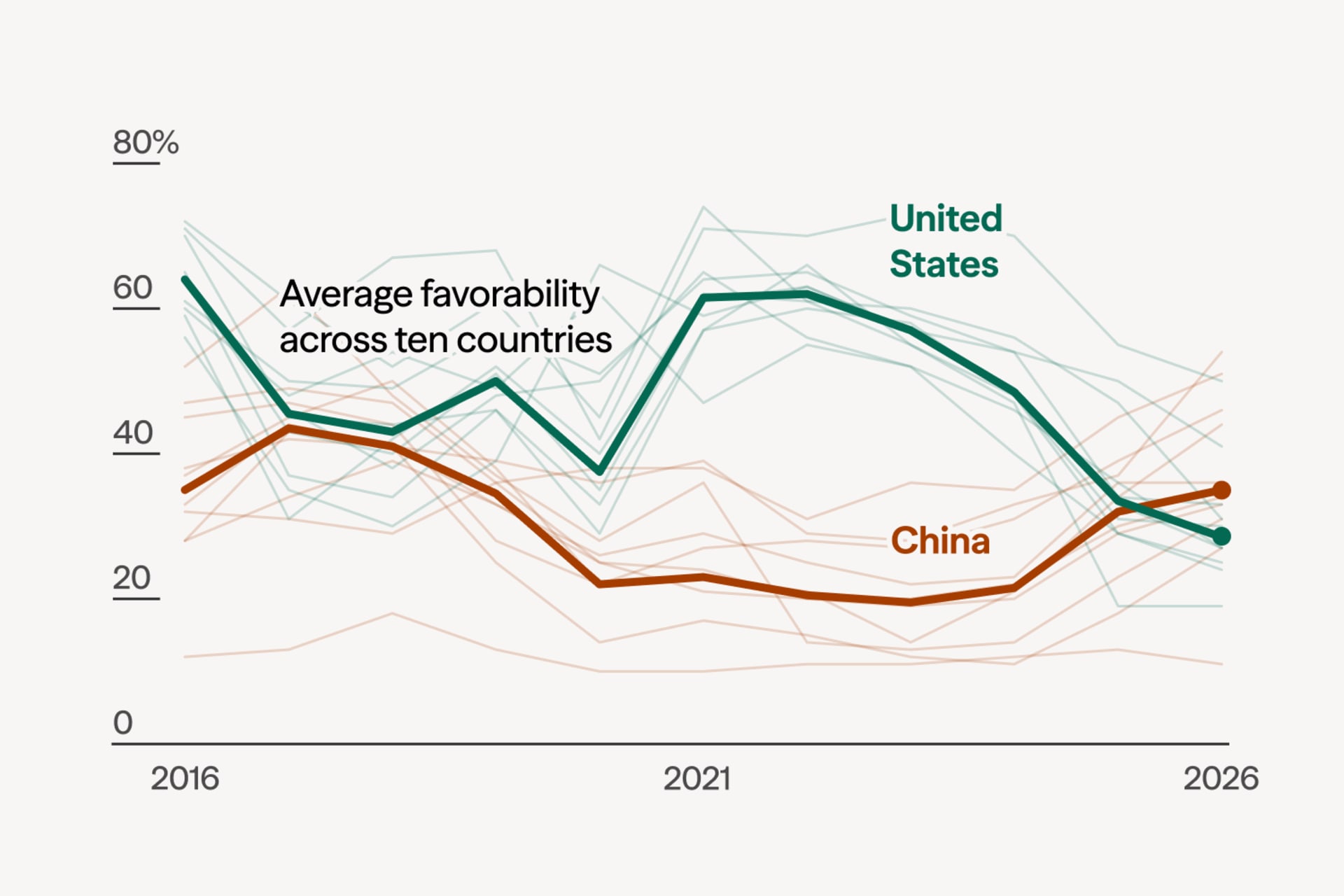
Survey Results: How AI Will Change the Global Balance of Power
The rise of AI means policymakers need to navigate a future defined by technological uncertainty. To help them do so, CFR asked foreign policy experts to predict how frontier AI capabilities and the governance structures that could emerge around them will affect the global order.
Around the World
CFR analyses and explainers that address global issues and challenges.
The Saudi Nuclear Deal Would Set a Dangerous New Proliferation Precedent
By Erin D. Dumbacher

The U.S.-Saudi Nuclear Deal Set Off Tremors. Is It Still Alive?
By Steven A. Cook

Andy Burnham: What to Expect From the UK’s New Prime Minister
By Matthias Matthijs and Benjamin Harris


Trump’s New Tariffs: What to Know
By Michael Froman

The ICC Has Real Flaws. Dismantling It Without an Alternative Is Not the Answer.
By John B. Bellinger III

250 Years of American Foreign Policy
 Expert Take
Expert Take Expert Take
Expert Take Expert Take
Expert TakeThe 10 Best and 10 Worst U.S. Foreign Policy Decisions
Council on Foreign Relations
Congress Checks Out
By Elliott Abrams
Where Does American Strategy Go From Here?
By Rebecca Lissner
The Coming AI Backlash
By Chris McGuire
Between Two Orders
By Charles A. Kupchan

After Hegemony
By Gideon Rose

Starting From Scratch
By Paul B. Stares

Overreach and Retrenchment
By Stephen Sestanovich

Podcasts
View AllThe Spillover
Every geopolitical event — a war, an election, a new tariff, a technological breakthrough — sends ripples through the global economy. On The Spillover, Sebastian Mallaby and Rebecca Patterson trace those ripples, examining how international developments shape markets, policy, finance, and the future of business.
 1:02:21Podcast
1:02:21Podcast

 51:39Podcast
51:39Podcast
Crisis Response Playbooks
The Wachenheim Center for Peace and Security has developed a set of Crisis Response Playbooks for U.S. policy planners when bandwidth is limited and decisions are consequential.


When armed conflict disrupts a critical maritime trade route, the United States can monitor, contain, or escalate the situation economically or militarily.


When a U.S. partner state faces a hybrid attack by an unknown aggressor, the United States should draw on various available response options to protect its treaty commitments, credibility, and commercial interests.


When a coup occurs abroad, the early hours of the crisis are most crucial for preserving and promoting U.S. interests—whether countering terrorism, checking adversaries‘ regional influence, upholding human rights norms, or maintaining diplomatic and economic relationships. Policy planners should therefore prepare for the unexpected.


Insurgency-related conflicts often start without warning and can last over a decade, making the pre-crisis and early crisis phases crucial for U.S. policymakers seeking to prevent national security threats and humanitarian disasters from emerging. Effective responses involve a complex set of legal authorities and international frameworks and require the sustained support of the American public and local communities.
CFR Events
View All





Publications
CFR publishes reports and papers for the interested public, the academic community, and foreign policy experts.


The Pharma Choke Point
Executive Summary U.S. dependence on China for essential medicines is structural—deeper, broader, and more consequential than conventional market analyses suggest. That dependence began with generic medicines and their ingredients but is now growing in biologics manufacturing, first-in-human trials, and synthetic DNA. That dependence is not simply the result of market conditions but rather decades of […]


Introduction Since the breakup of the Soviet Union, Russia has made a concerted effort to keep Belarus in its sphere of influence. Belarus’s political, economic, and military autonomy has ebbed and flowed over time, depending on geopolitical circumstances, Russia’s needs, and Belarusian President Alexander Lukashenko’s political adroitness. Nevertheless, the present moment poses unique challenges for […]


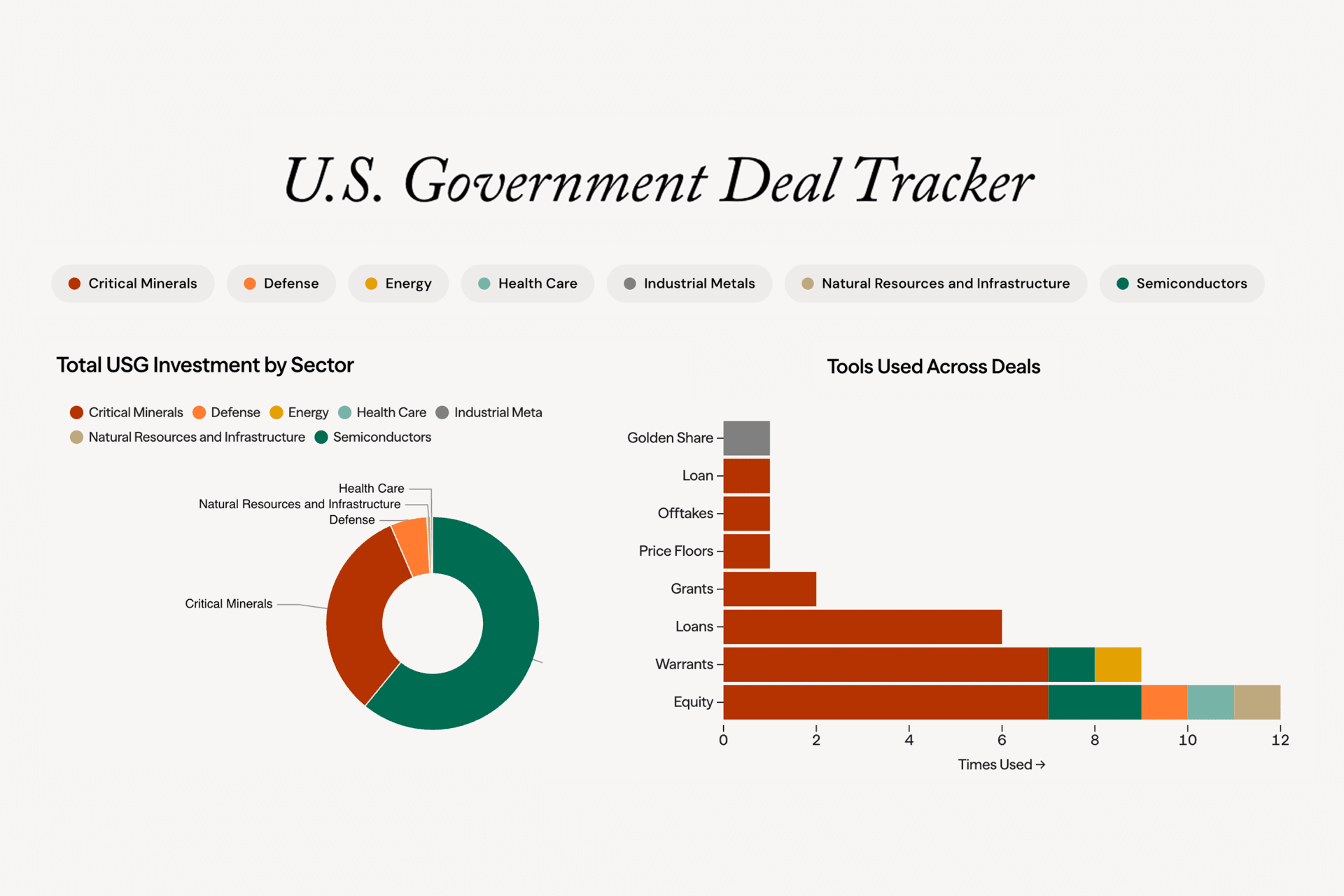
CFR’s U.S. Government Deal Tracker shows how the government is experimenting with new tools and financing structures to advance a range of strategic sectors, including critical minerals, energy, global logistics, manufacturing, telecommunications, and other technologies.
By Jonathan E. Hillman


A gap in private funding for companies and projects inhibits energy innovation in the United States. This “missing middle” slows or blocks technologies that could help the energy system become more secure, affordable, reliable, and sustainable from advancing through the demonstration and scale-up stages. Recent events have made the missing middle wider.


Suzanne Maloney, vice president and director of the Brookings Institution’s Foreign Policy Program, recommends that the United States reconsider its assumptions around eventual leadership change in Tehran, revive regime accountability efforts, prepare for opportunistic escalation by proxy groups, and ready itself for renewed nuclear diplomacy.


CFR International Affairs Fellow in National Security Roxanna Vigil argues that the United States should engage early with Colombia’s next administration to signal support for full implementation of the 2016 Peace Accords and provide targeted assistance.


The United States cannot out-mine and out-process China. Instead, it should leapfrog China’s dominance by scaling disruptive innovation, recovery, and recycling.
CFR in the News
View All
15 Books Longlisted for 2026 Cundill History Prize
Quill & Quire



The weaponisation of trade
Financial Times

When the dollar became a weapon
Blockworks Daily
Latest Content
View AllExpert Take Expert Take
Expert Take Expert Take
Expert Take